
Endobronchial Blockers for Lung Isolation in Massive Hemoptysis
Introduction: Balloon-based endobronchial blockers were developed for lung isolation for thoracic surgical procedures as an alternative to double lumen intubation. They have been used, however, for lung isolation in the setting of massive airway bleeding . There are a variety of endobronchial blockers available on the market, which vary in regards to design and instructions for u se. The purpose of this essay is to describe the basic specifications and techniques for using two such devices as they may be applic able to clinicians encountering massive airway bleeding.
Background: Most patients with massive hemoptysis die due to asphyxiation. Approximately 150 to 200 milliliters (ml) of blood could interfere with gas exchange and cause respiratory failure and death. This is because the amount of blood needed to fill the anatomical dead space in most patients is only about 150 ml. Massive hemoptysis has been defined in different series as > 200 to >
600 mL of blood per 24 hours, but due to the rather small quantity of blood needed to fill the anatomic dead space, death wil l typically occur prior to exsanguination. Bleeding rate of ≥ 1,000 ml within a 24-hour period, aspiration of blood in the contralateral lung, massive bleeding requiring single-lung ventilation and lung cancer as underlying etiologies have all been associated with higher mortality. Morbidity and mortality are reportedly less when tuberculosis, bronchitis or bronchiectasis were responsible fo r the massive hemoptysis. Some series report higher mortality rates in patients who experienced recurrent bleeding following bronch ial artery embolization (BAE) for massive hemoptysis.
The first priority in the management of massive hemoptysis is to maintain a patient airway. While setting up the equipment fo r endotracheal intubation and lung isolation, the patient should be placed in the lateral safety position (lateral decubitus po sition) with the bleeding side down so blood does not also fill the unaffected lung. Bronchoscopists should be familiar with the use of endobronchial blocker placement as a means to isolate the bleeding lung, control massive hemoptysis and spare airways for gas e xchange. In fact, transporting a patient to interventional radiology or intensive care unit without a secured airway (and isol ated bleeding lung) in cases of massive hemoptysis is considered unsafe in the event of airway occlusion from large blood clots in route. Commonly used endobronchial blockers mainly vary in steering technique, balloon size, locking mechanism and method of placement. The two blockers described herein need visual guidance for proper placement in the desired airway. A locking system is available to secure the blocker in the desired location and reduce the risk for migration. There are no published surveys, ho wever, assessing the operators’ comfort level or user-friendly features for the various available systems. The Arndt endobronchial blocker (Cook Medical) require the use of a pediatric bronchoscope when the blocker is placed though a regular 7.0 -8.5 endotracheal tubes. An alternative technique can be used, in which the blocker can be inserted in the airway alongside the endotracheal tu be, even by using a regular diagnostic adult bronchoscope (Figure1). The VivaSight –EB (Ambu A/S) can be used without the bronchoscope when inserted through a dedicated endotracheal tube with a built-in camera (VivaSight –SL, Ambu A/S) (Figure 2). To date, there are no comparison studies between the blockers designed by different manufacturers. Familiarity, availability, the feas ibility of using a bronchoscope in emergent situations and costs impact operators’ selection of a particular endobronchial blocker.
Clinical applications: The Arndt endobronchial blocker (Cook Medical) and the VivaSight-EB (Ambu A/S) while approved for clinical use for lung isolation, have not yet been systematically studied for massive hemoptysis. There are several issues that requir e attention when using these devices for lung isolation in massive hemoptysis:
- Massive bleeding from the left lung: selective intubation of the right main bronchus (RMB) should be performed emergently.
However, because of the short length of the RMB (1.5-2 cm), it is very likely that the takeoff of the right upper lobe bronchus
would be occluded if the ETT is properly positioned in the RMB. Ventilation to the right lower lobe (RLL) and right middle lo be (RML) may not be tolerated, and thus, alternatives have been proposed; a double lumen endotracheal tube could be considered, but it may not be feasible to place these tubes in emergent situations for hemoptysis. Thus, an endobronchial blocker could be placed in the left main bronchus, while keeping the ETT in the trachea (Figure 3). This way, the entire right lung i s being ventilated, while preventing spillage of blood from the left lung. - Massive bleeding from the right lung: in this scenario, the left lung should be selectively intubated; this is feasible as the left main stem bronchus is typically 5 cm in length and a single lumen ETT can be placed in positioned in the LMB. If the bleeding is from the RML or RLL, however, the ETT can be secured in mid trachea and the blocker positioned in the Bronchus intermedius (Figure 1), allowing ventilation not only of the left lung but also of the RUL.
- Patient safety during and blocker insertion:
A. The balloon should never be overinflated; in fact, the balloon should be deflated for a few minutes three times a day in o rder to preserve mucosal viability and to check for bleeding recurrence.
B. If ventilation becomes difficult during endobronchial blockade, the balloon should be deflated and the its position inspec ted as migration is possible
C. Higher PEEP and low tidal volume may occur during placement due to the presence of scope and blocker in the ETT
Conclusions: The available endobronchial blockers have different design, insertion technique and maneuverability. The lack of published literature makes a fair comparison between different blockers in the same patient population impossible. We believe that by a ppropriately using the endobronchial blockers in the setting of massive hemoptysis, practitioners can safely isolate the bleeding lung and potentially stabilize patients until definitive treatment is offered.
Figure 1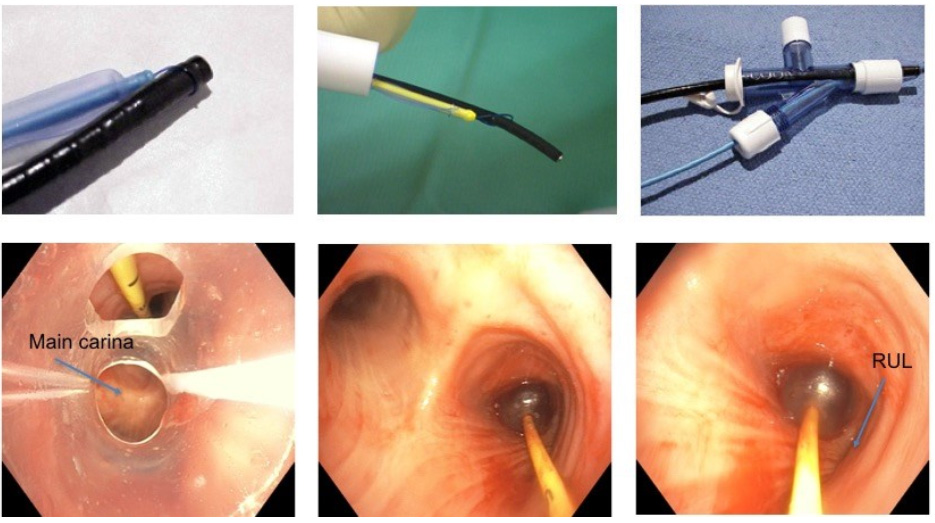
Arndt Endobronchial blocker. Top left: The Arndt endobronchial blocker uses a guide loop assembly that fits through the lumen of the blocker and exits from the blocker’s distal end to form a small, adjustable loop. Top center: The bronchoscope is placed through the diaphragm of the bronchoscopy port of the Arndt Multiport Airway Adapter; the bronchoscope is advanced through the guide loop. Top right: Once coupled through the Arndt Multiport Airway Adapter, the bronchoscope and the blocker are placed
on the endotracheal tube and the patient ventilated with 100% oxygen. The guide loop should be adjusted to loosely approximate the diameter of the bronchoscope. Bottom left: The blocker is inserted in the airway alongside the endotracheal tube. Bottom Center: The blocker can be placed in the bronchus intermedius (BI) in cases of bleeding form the RML or RLL. Bottom right: When placed in the BI, the RUL bronchus patency is maintained. Photos courtesy of Eric Edell, Mayo Clinic and Septimiu Murgu, University of Chicago.
Figure 2
Left panel: VivaSight-EB is an endobronchial blocker designated for lung isolation. It consists of a
sterile, single-use, “steerable” balloon-tipped catheter that is visually guided to a selected airway. The angled distal tip of VivaSight-EB can be adjusted to facilitate placement in the desired bronchi. When used in conjunction with the VivaSight-SL continuous monitoring throughout the procedure ensures that dislocation can be easily detected and corrected.
Right panel: For visual guidance during positioning the blocker can be used in combination with the bronchoscope or the VivaSightSL single lumen tube (arrow) with integrated camera.
Figure 3
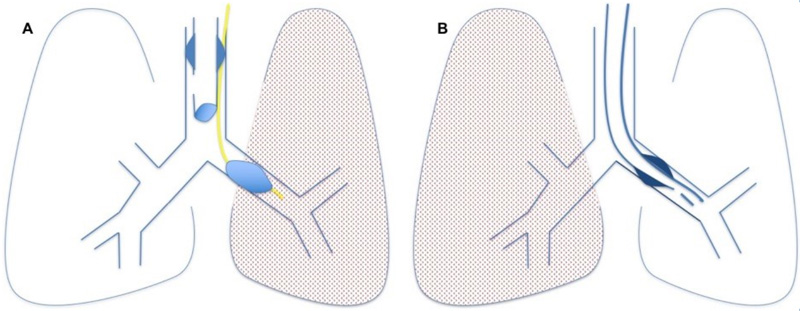
Managing strategies for massive hemoptysis. A. In case of left lung bleeding, the ETT can be secured in the trachea and the endobronchial blocker placed either through the ETT or along its side and positioned in the left main bronchus. The right upper lobe can be closed off with a right mainstem bronchus intubation. B. In cases of right lung bleeding, the left main bronchus can be intubated over the bronchoscope. This is possible as the LMB is ~5 cm in length.
References
1. Sakr L et al. Respiration 2010; 80: 38-58
2. Shigemura N et al. Ann Thorac Surg 2009;87:849–853.
3. Conlan AA et al. Thorax 1980; 35:901-9044.
4. Kalyanaraman M et al. Otolaryngol Head Neck Surg 1997; 117:56-61.
5. Dweik R et al. Clin Chest Med 1999; 20:89–105
6. Garzon AA, et al. Ann Surg 1978;187:267–271
7. Osakia SI et al. Respiration 2000;67:412–416. 49
8. Wang GR et al. J Vasc Interv Radiol 2009;20:722–729. 50
9. Van den Heuvel MM et al. Int J Tuberc Lung Dis 2007;11:909–914









