
Robot-Assisted Bronchoscopy
Introduction
The use of robots in medicine has been around for 35 years, with the first “robot surgeon” used on a human patient being PUMA 2000 in 1985, to perform CT guided neurosurgical biopsies. In 1990’s, scientists developed a robot with remote manipulators controlled by a surgeon for laparoscopic surgeries [1]. Since then, robotics has been used in the field of general surgery, gynecologic surgery, and urological surgery as well as cardiac and thoracic surgery. Robotic thoracic surgery offers multiple advantages over traditional Video Assisted Thoracoscopic Surgery (VATS) such as increased 3-D visualization, increased degrees of freedom of motion, better ergonomics and increased precision and in 2011 comprised approximately 10% of all lobectomies in the United States [2]. In the field of thoracic oncology, the increasing need to efficiently and safely sample lung lesions, has led to the development of guided bronchoscopy systems such as virtual bronchoscopy (VB), radial endobronchial ultrasound (r-EBUS) and electromagnetic navigation (EMN). The diagnostic yield of guided bronchoscopy using EMN ranges from 67-84%, with a one year follow up of the NAVIGATE study showing a diagnostic yield of 73% [3], but is lower than CT-guided transthoracic needle aspiration (92.1%) [4]
The lower diagnostic yield may be explained by the following factors which can be potentially overcome by using the newly available robot-assisted bronchoscopic (RAB) systems. Some bronchoscopists may get disoriented beyond the 5th generation airways and miss a small peripheral airway leading to the lesion. The use of EMN has been combined with r-EBUS to increase diagnostic yield, but can be limited by respiratory motion and CT-to-body divergence. The RAB technology allows the operator to navigate through smaller airways under direct visualization while continuing to offer either EMN guidance (MonarchTM platform by Auris Health Inc.) or Fiberoptic Sensing Navigation (IonTM Endoluminal System by Intuitive Surgical) to find target airways and also provides stability during sampling of the target lesion.
Background
There are currently two commercially available RAB platforms on the US market. The MonarchTM platform by Auris Health Inc. was FDA approved in March 2018. In cadavers, the Monarch TM platform was noted to have farther access to the periphery of the lung when compared to a conventional thin (4.2mm OD) bronchoscope (9 vs 6 airway generations) [5]. Rojas-Solano et al performed the first feasibility study with the Monarch TM platform in 15 patients that showed no pneumothoraces or significant bleeding [6]. The IonTM Endoluminal System by Intuitive Surgical was approved by the FDA in February 2019. Fielding et al. demonstrated that the IonTM system safely navigated to very small peripheral airways under direct visualization in 29 subjects, and were capable of biopsing small solitary pulmonary nodules while maintaining a static position [7]. The differences between the two available robotic systems are highlighted in Table 1.
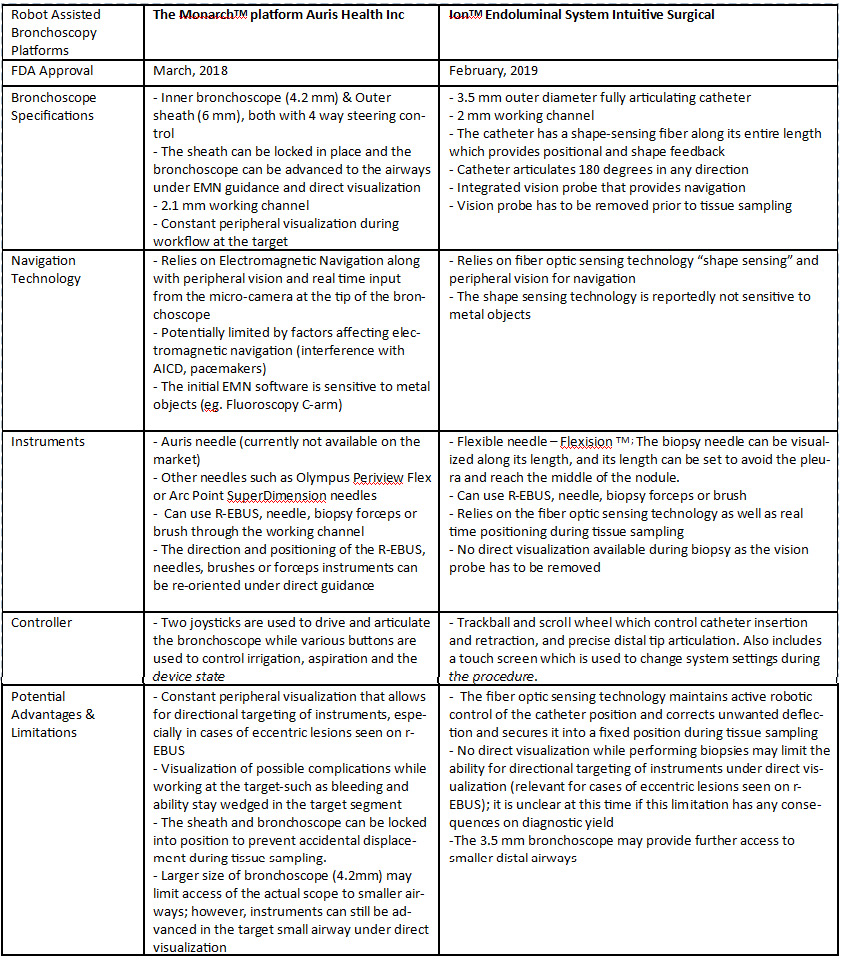
Table 1. Comparison of the MonarchTM platform and IonTM Endoluminal System
Clinical Application
For peripheral lung lesions sampling, robotic platforms may overcome some limitations of the currently available guided bronchoscopy systems. These systems may increase the diagnostic yield due to their stability, adjustable angulation and peripheral visualization, when available. A retrospective post-marketing study by Chaddha et al. showed that the Monarch TM robotic platform was used in 82 cases to successfully navigate to 90.2% of the lung nodules (79.3% located in the outer third of the lung) [8]. Chen at al. in a multicenter prospective study demonstrated lesion localization in 91.7% cases also using the MonarchTM Auris robotic platform [9]. Both of these studies (presented in an abstract form) did not report the diagnostic yield as the follow up period post intervention was not sufficient for defining true negative cases. Fielding et al. recently published the first study using the IonTM Endoluminal System showing an overall diagnostic yield of 79.3% and a diagnostic yield for malignancy of 88% [7]. Both of these studies suggest that RAB is a feasible technology with low adverse events that has the potential of increasing the success of navigation and diagnostic yield in patients with peripheral nodules.
In addition to their potential for improving diagnostic rates, robotic bronchoscopies may guide ablative therapies for treating inoperable peripheral lung tumors or oligometastatic lesions. Animal and case studies in humans have demonstrated feasibility of guided bronchoscopic ablative therapies such as laser interstitial thermal therapy [10], photodynamic therapy [11] radiofrequency ablation [12], microwave ablation [13] and bronchoscopic thermal vapor ablation. Robotic assisted bronchoscopy may further increase the accuracy in guiding flexible catheters to peripheral lesions and provide a stable platform to deliver ablative therapies [14, 15]. It is, however, premature to say that any of these therapeutic modalities are ready for clinical use. A few questions that will have to be answered by future research include but are not limited to: What are the exact energy settings to be safely applied during peripheral MWA? How many fibers should be used for peripheral PDT? Is concentric location of the probe essential for reliable ablation? What is the optimal location and freezing time for peripheral cryoablation?
It is possible that these interventions will have to be performed under direct imaging guidance (maybe cone-beam CT) for precise application of the probes and for monitoring intra-procedural effect.
Conclusions
The currently available small studies suggest that RAB is feasible and safe, but further data are needed to determine whether these technologies improve the diagnostic yield when compared to current bronchoscopic-guided diagnostic modalities. In these authors’ opinion, the vast majority of patients with suspected lung cancer require concurrent EBUS-TBNA either because of the primary lesion size, location, presence of intrathoracic adenopathy on CT or PET or prior to stereotactic body radiation therapy.
Auris Health, Inc. is currently conducting a multi-center prospective trial to study navigation success and diagnostic yield in patients with peripheral pulmonary lesions using the MonarchTM platform (https://clinicaltrials.gov/ct2/show/NCT03727425). An ongoing multi-center single arm study is evaluating early outcomes associated with the IONTM Endoluminal System looking at navigation success, biopsy success as well as diagnostic yield trends in patients with lung nodules (https://clinicaltrials.gov/ct2/show/NCT03893539).
If the studies using RAB reliably demonstrate the ability to reach peripheral lesions as confirmed by radial EBUS or cone beam CT, RAB could eventually play a role in guiding ablative therapies for inoperable primary lung tumors or oligometastatic lesions.
References
- Ghezzi TL et al. World J Surg.2016 40: 2550
- Novelis P et al. J Thorac Dis 2018 Feb; 10(2): 790–798.
- Folch E et al. J Thorac Oncol. 2019 Mar;14(3):445-458
- DiBardino D et al. J Thorac Dis. 2015; 7(Suppl 4): S304-S316
- Chen AC et al. Ann Thorac Surg. 2018 Jul; 106(1):293-297
- Rojas-Solan JR et al. J Bronchology Interv Pulmonol. 2018 Jul; 25(3):168-175.
- Fielding et al. Respiration. 2019;98(2):142-150
- Chaddha U et al. ARJCCM 2019;199:A1266
- Chen AC et al. ARJCCM 2019;199:A7304
- Casal RF et al. J Bronchology Interv Pulmonol. 2018;25(4):322-329.
- Musani A et al. Lasers Surg Med. 2018;50(5):483-490.
- Koizumi T et al. Respiration. 2015;90(1):47-55.
- Howk K et al. AJRCCM 2016;193:A6019.
- Chaddha U et al. Ann Am Thorac Soc. 2019 Jun 13. doi: 10.1513/AnnalsATS.201812-892CME.
- Murgu SD. BMC Pulmonary Medicine. 2019;19(1):89
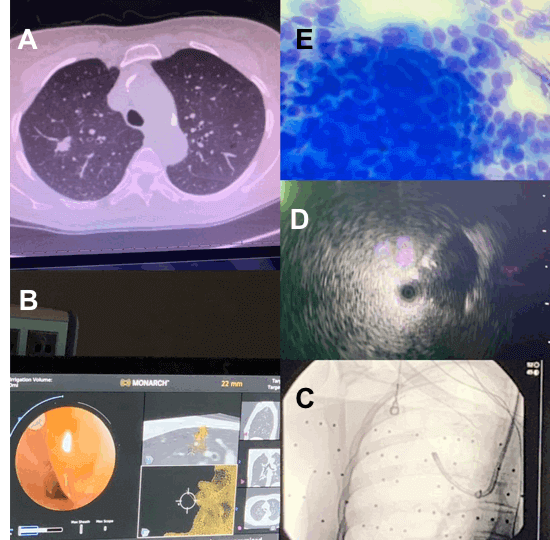
Figure 1: MonarchTM platform by Auris Inc.
A. Computed Tomography (CT) image of the right upper lobe nodule. .
B. Real time white light bronchoscopy view and target view on the MonarchTM platform. .
C. Fluoroscopic image of robotic bronchoscope..
D. Eccentric radial EBUS view of peripheral pulmonary nodule..
E. Diff quick stain from needle aspirate (RUL nodule) showing non-small cell lung cancer.
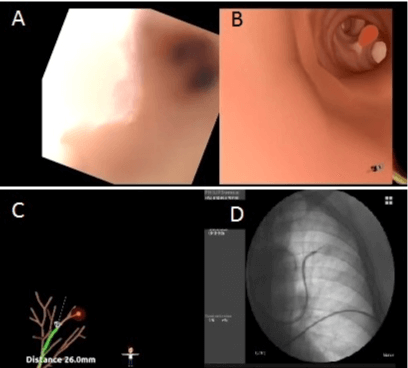
Figure 2: IonTM Endoluminal System by Intuitive Surgical (Courtesy of David Fielding, MD, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia)
A. Real time view using the vision probe.
B & C. Global view with shape-sensing fiber displaying the position of the catheter in the airway and distance from target lesion.
D. Fluoroscopic image demonstrating catheter position.









