Bronchoscopic Lung Volume Reduction Techniques and Pitfalls of Placing and Adjusting Endobronchial Valves
Hyperinflation is one of the most devastating consequences of COPD, especially those with an emphysematous phenotype.1 It correlates with increased breathlessness, decreased exercise performance, worsened quality of life, respiratory failure, hospitalization and in those most hyperinflated, it is a major risk for mortality.2 Lung volume reduction surgery (LVRS) in carefully selected individuals with hyperinflation and advanced emphysema has shown to be beneficial in improving lung function, exercise performance and quality of life, and in a subset with upper lobe predominate disease and ventilatory limited exercise, survival.3 Despite the positive benefits of LVRS on patient outcomes, its perceived high morbidity and mortality and costs of care coupled with limited availability has relegated it to less than 200 Medicare beneficiaries with emphysema receiving that therapy on an annual basis.4 For the last 2 decades, multiple bronchoscopically placed devices using a variety of techniques have been developed to duplicate the effects of LVRS on deflating the lungs of hyperinflated patients with advanced emphysema. Although these techniques differ markedly from one another, they all share the main objective to decrease thoracic volume and thus improve lung, chest wall, respiratory muscle and cardiac performance.3,5-7
Several of these techniques are shown in Figure 1; endobronchial valves have received FDA approval for clinical use in properly selected patients with hyperinflation due to emphysema and the absence of collateral ventilation. The other therapies are not approved for clinical care in the U.S. and some (lung coil, Aeriseal, vapor ablation) are either undergoing clinical trial evaluation, or have limited clinical access (lung coil, vapor ablation) outside the U.S. For those reasons, I will focus on the techniques and practices of placing and removing endobronchial valves.
1. Patient selection. Patient selection is key for which patients to treat, and which lobe to treat with endobronchial valve (EBV) therapy.8,9 All patients should be maximally medically treated with maximal bronchodilator therapy, supplemental oxygen if criteria are met and use of pulmonary rehabilitation or evidence of an active lifestyle. Dual long acting bronchodilators, supplemental oxygen and rehabilitation all have been shown to attenuate air trapping by either decreasing airways resistance or respiratory rate, respectively, thus prolonging expiration and decreasing air trapping.10 Patients morbidly obese (BMI > 34) or severely undernourished (BMI < 19) should have nutritional status optimized before considering an EBV procedure.
Patients selected for EBV should have advanced emphysema and suffer from hyperinflation. Lung function testing should demonstrate that patients have severe airflow obstruction (FEV1 15-45% predicted), hyperinflation (TLC >100%) and air trapping (RV >150% predicted). Additionally, patients should not have severe gas exchange imbalance (PaO2< 45 mmHg, PaCO2 > 50-55mm Hg, DLCO < 15% predicted, O2 requirements > 6L at rest or with ambulation).8,9
Patients should not have uncontrolled or severe comorbid conditions that may be contributing to their symptom burden of breathlessness or provoke significant periprocedural or post procedural complications. Patients with coronary artery disease or severe pulmonary hypertension should be avoided, uncontrolled or poorly controlled supraventricular tachycardias or symptomatic CHF or low EF states should be avoided. Hematologic abnormalities or the need anticoagulation needs to be addressed to ensure that constant anticoagulation is not needed during or immediate post procedure when urgent chest tube placement may be needed.
All patients referred for EBV have multidisciplinary assessment for lung volume reduction surgery or lung transplantation, the full array of interventions is individualized for what the patients’ needs are at that time and stage of their disease while always attempting to balance the risks and the benefits.
2. Selecting the lobe for EBV treatment. EBV is only effective when total lobar occlusion leads to a significant decrease in targeted lobe volume reduction, at least 350 ml reduction. Most studies should that this can be achieved in about 70-80% of patients if the following selection criteria are used: a) more than 40-50% destruction of the EBV target lobe, b) fissure integrity or lack of physiologically determined endobronchial airflow between the targeted lobe and ipsilateral non treated lobe, c) greater inspiratory lobar volume, and d) decreased lobar perfusion. Additional considerations should include the degree of heterogeneity between the target and ipsilateral non targeted lobe- a greater difference may indicate a better treatment response, picking a lung to treat that lacks evidence of pleural adhesions, lung nodules, significant bronchiectasis or interstitial infiltrates.11 The pattern of emphysema needs to be considered- those with predominately pre pleural emphysema may benefit from surgical resection of peripheral emphysema areas rather than sacrificing functional parenchyma with EBV total lobar occlusion.12 In homogenous cases, a perfusion assessment is recommended to select a lobe that is less than 20% perfused compared to other lung lobes.13 Depending upon an individual patient’s anatomy, multiple targets may be possible, preplanning the procedure to prioritize the lobar targets that achieve the removal of the greatest volume of dead space is recommended.
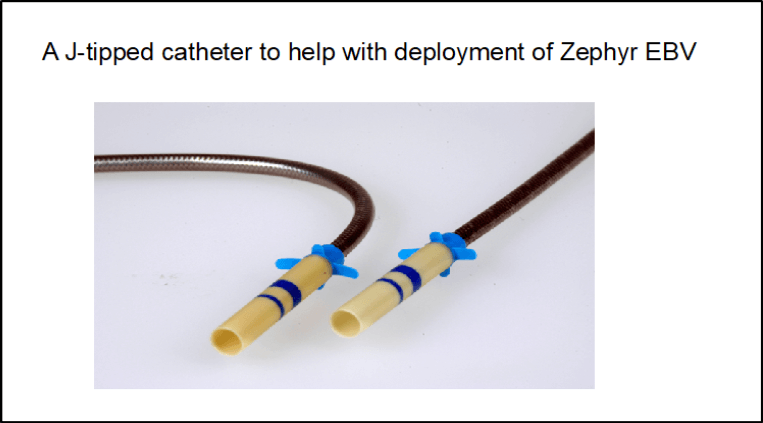
3. EBV placement. During the procedure, an airway examination is performed to exclude any endobronchial lesions, suction any secretions and if purulence is found submit for microbiological culture. Assessment of collateral ventilation can be performed using a balloon tipped catheter inserted via the bronchoscope and inflated into the target or non-targeted lobe to asses flow across a major fissure.8,14 Alternatively, analysis of a pre procedural HRCT analyzed for fissure integrity has been reported to be effective in selecting the lobe for EBV treatment.9 The segmental orifices in the lobe targeted for EBV treatment are then sized for EBV length and width using either a calibrated balloon or using an unloaded deployment catheter with flap-tabs that measures airway width.(Figures 2 and 3) Airway length is sized with calibrated markings on the catheter shaft.(Figure 2) Sizing is recommended to be sequential after EBV placement- some configurational changes may be made in the airway dimensions once an EBV is placed in the adjacent orifice. Care should be taken that the EBV is inserted parallel to the airway wall to prevent rotational changes or development of granulation tissue and that the valve is seated with its struts below the segmental orifice and the valve structure occludes the orifice without gaps, overdistention or protrusion of the valve structure outside of the airway orifice. In some difficult to access segments, a j-wire device may be used to deploy the EBV or using ventilator inflation hold, change in head or body position may also enable better access during deployment.(Figure 4) Post procedure instillation of saline should be done to assess for any bubbles that may emanate around the valve border with the airway wall indicating lack of lobar occlusion. We perform a pre and post procedural ultrasound of the intended lung and lobe of treatment to demonstrate absence of sliding after EBV therapy in the target lobe and continued sliding in the ipsilateral non targeted lobe to indicate lobar occlusion of the target lobe and no evidence of pneumothorax post procedure.
4. Post procedural assessment. At our institution we perform a CXR post procedure on the table, at one and 3 and 8 hours post and then daily till discharge. We keep patients hospitalized for 4 nights and see them in clinic at one-week post discharge with a CXR and 6-minute walk test for oxygen assessment. At day 45 we perform a HRCT to assess for target lobe volume reduction and if less than 50% targeted lobe reduction we consider repeat bronchoscopy with valve adjustment based on any changes in valve position identified by HRCT or lack of clinical response.8 Valves are easily removed by using forceps remembering to remove the EBV from the orifice by rotating it out of the airway before withdrawing it into the central airway. Sizing is then performed as previously mentioned. On repeat examination if significant granulation tissue is present, we remove it with directed cryotherapy or APC treatment. We then perform HRCT annually to assess for treatment effect and lung cancer surveillance based on prior smoking history and age according to published recommendations.
5. Long term goals of EBV treatment. Treatment of hyperinflation is the goal of effective EBV, patients with total lobar collapse may have a survival benefit based on some cohort single center studies. Emphysema is a progressive disease, EBV is only one part of an individual patient’s treatment regime to reduce hyperinflation, other medical and non-pharmacologic treatments such as supplemental oxygen and physical activity need to continue. Some patients may move on to transplant or in case where EBV is not successful lung volume reduction surgery. A successful EBV program should follow and assess the patient’s outcome longitudinally to optimize outcome post EBV and more importantly improve the patient’s long-term trajectory of this devastating disease.
References
- Langer D et al. Expert Rev Respir Med. 2014;8(6):731-749.
- Casanova CP et al. Am J Respir Crit Care Med. 2005;171(6):591-597.
- Criner GJ, et al. Am J Respir Crit Care Med. 2011;184(8):881-893.
- Marchetti N et al. Semin Respir Crit Care Med. 2015;36(4):592-608.
- Criner G et al.. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1578-1585.
- Criner GJ. Chest. 2010;138(1):6-8.
- Criner RN, et al. Chronic Obstr Pulm Dis. 2018;6(1):40-50.
- Criner GJ et al. Am J Respir Crit Care Med. 2018;198(9):1151-1164.
- Criner GJ et al. Am J Respir Crit Care Med. 2019.
- Di Marco et al. Respir Res. 2018;19(1):18.
- Sciurba FC et al. N Engl J Med. 2010;363(13):1233-1244.
- Valipour A et al. Respiration. 2015;90(5):402-411.
- Valipour A et al. Am J Respir Crit Care Med. 2016;194(9):1073-1082.
- Gompelmann D et al. Respirology. 2014;19(4):524-530.
Figure 1:
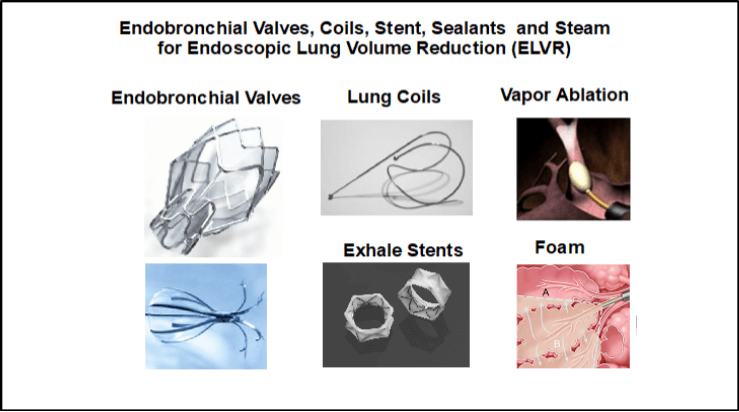
Figure 2:
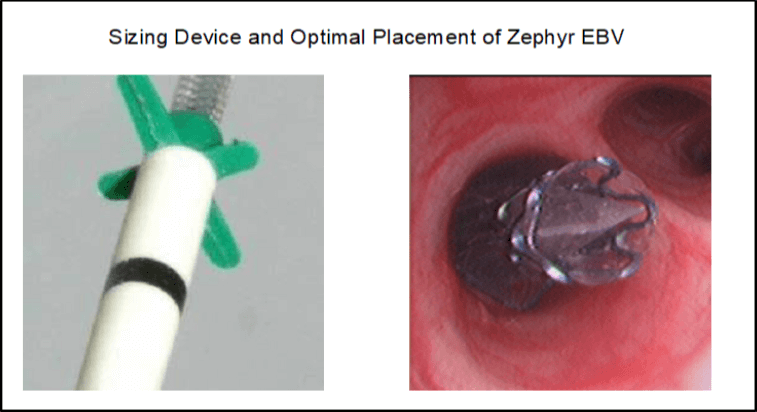
Figure 3:
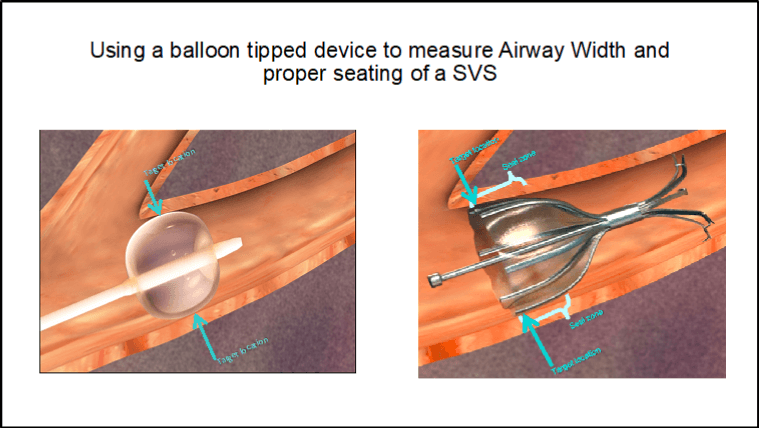
Figure 4: