
Spray Cryotherapy

Ganesh Krishna, MD, FCCP
Professor of Medicine, University of California, San Francisco.
Interventional Pulmonologist, Palo Alto Medical Foundation.
Airway recanalization is generally attempted to provide palliation for symptoms (1) due to lung volume loss and hypoxemia. It is also done to decrease the likelihood of a significant airway hemorrhage leading to blood loss or drowning. Relief of mechanical airway obstruction also reduces the likelihood of post obstructive pneumonia. The majority of airway recanalizations are done for malignant airway obstruction. However, patients with non-malignant airway obstructions may also derive benefit (2). Airway recanalization modalities broadly fall into two categories: heat based and cold based. Examples of heat based recanalization devices include Laser and Argon plasma coagulation. Examples of cold based recanalization devices include cryo spray ablation and flexible cryo probe. Mechanical debriders such as rigid bronchoscopy and micro debrider bronchoscopy are also available. A combination of these modalities are used commonly to achieve palliative goals. Heat based recanalizations require the airway FiO2 to be less than 0.4 to avoid airway fires. Gas embolism is also a potential complication of argon plasma coagulation. It is beyond the scope of this article to discuss all modalities of airway recanalization. We will focus on cryo spray ablation for central airway obstruction.
Spray cryotherapy (SCT) is a relatively new modality available to the trained interventional pulmonologist or thoracic surgeon as a reliable tool in providing palliative airway recanalization to a carefully selected patient. The third generation truFreeze system (CSA medical, Lexington, MA, USA) is approved for airway applications. This system uses liquid nitrogen as the cryogen and is delivered through a specialized braided catheter that is compatible with the working channel of a standard therapeutic bronchoscope. The liquefied gas is delivered through the catheter at low pressure (2-4 PSI). The gas expands 700 fold after exiting the catheter and drops the temperature to -196⁰ C, thereby providing the desired effect on tissue. Therefore, allowing egress of the gas is of paramount importance to avoid barotrauma.
SCT is a temperature dependent modality that is shown to be safe and effective in the treatment of central airway obstruction (CAO). It utilizes flash freezing of tissue at a temperature of approximately 196⁰ C, resulting in non-contact cell death of tissue with relatively high water content (malignant cells, granulation tissue). Anhydrous tissue such as extracellular matrix and collagen that are an important component of airway tree is spared, making it a desirable tool for airway recanalization (3). Regenerative growth of tissue is also not impaired. Targeted delivery of low dose liquid nitrogen with 2 cycles of 5 second duration has been shown to cause tissue damage of up to 1.5 mm in the human airway (4).
Patients with symptomatic central airway obstruction (CAO) due to malignant or non-malignant disease processes are candidates for Cryospray ablation (5). Patients should be able to tolerate general anesthesia. It is preferred that in most cases a rigid bronchoscope be used to allow passive venting of nitrogen. However, a flexible bronchoscope with an endotracheal tube can also be safely used in patients who are unable to tolerate rigid bronchoscopy. In our institution, we undertake specific precautions when we use a flexible bronchoscope: we deflate the cuff of the endotracheal tube during activation and use an endotracheal tube with a subglottic port connected to a suction tubing for active venting of nitrogen. The endotracheal tube is stabilized with a mouth guard that holds the tube in position when the cuff is deflated. In both situations, the patient is disconnected from the ventilator during activation. Airway FiO2 need not be adjusted for this procedure. Transient desaturations is not uncommon as nitrogen displaces oxygen from the pulmonary circuit but recovery is usually quick. We recommend not more than five to seven activations per site in the tracheobronchial tree. Visual and tactile verification of gas egress is important. The device is used as a noncontact form of tissue destruction. The catheter is passed approximately a centimeter distal to the working channel of the bronchoscope. After the nitrogen is activated with a foot pedal, shortening of the catheter is observed followed by circumferential ice formation. The timer is started at this point for 5 seconds and counts as an activation. Two settings, low and medium flow are available to the operator. We strongly recommend having trained support staff. Palpation of the chest wall and neck for crepitus after each activation will also allow early recognition of potential complications. Gas embolism has not been reported with SCT.
Proximal tracheal lesions present a specific challenge for airway recanalizations in general and particularly with SCT. Given the proximity of the entrance of the gastrointestinal tract, there is a significant risk of gas egress into the GI tract causing visceral organ damage or rupture. Proximal tracheal lesions are usually addressed with laryngeal mask airway (LMA) or suspension laryngoscopy, as rigid bronchoscopy and endotracheal tube is not practical. Access to physicians trained in suspension laryngoscopy and the equipment itself is not readily available in most institutions. In our institution, we devised a method by which we use an esophageal balloon to occlude the proximal GI tract and were able to successfully perform SCT on patients with proximal airway obstruction with laryngeal mask airway (accepted for publication, with revisions). We used a 5.5 cm esophageal balloon (Merit Medical Endotek, South Jordan, UT) and inflated it to 12 mm at 8 ATM pressure to fully occlude the esophagus to prevent nitrogen entry into the gastrointestinal tract. In addition, a dedicated staff member was asked to palpate the abdomen for distension during activation as an extra precaution.
We view SCT as one of the myriad tools available for airway recanalization for malignant or non- malignant CAO. It can be used as a standalone device or in conjunction with other tools. Specialized training is necessary for the operator as well as support staff. In trained hands and carefully selected patients, it is a valuable tool that provides long lasting palliation of symptoms caused by airway obstruction.

Figure 1: Cryo spray therapy console
|
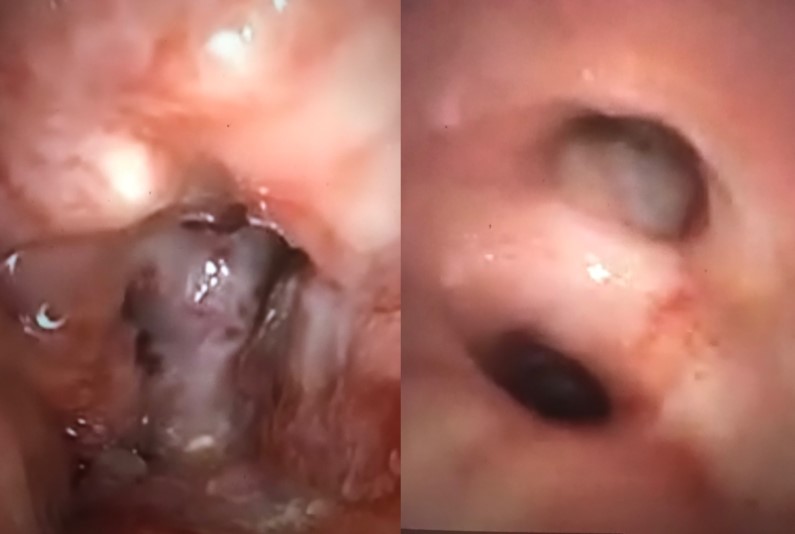
Figure 2: Pre treatment and 6 weeks post treatment
|
References
- Mahmood et al. Respiration. 2015; 89(5): 404-413.
- Bhora et al. Head Neck Surg. 2016; 42(11): 1082-1087
- Gage et al. Cryobiology. 1998; 37(3): 171-186.
- Krimsky et al. J Thorac Cardiovasc Surg. 2010; 139(3): 781-782.
- Finley et al. Ann Thorac Surg. 2012; 94 (1): 199-203.









